



learn what other specialties are part
of the cardiometablic medicine industry

Join the movement and share your story on social media. Don't forget to use the hashtag #IamCardiometabolicMedicine
#IamCardiometabolicMedicine
Elevate your knowledge, skills, and practice with our
world class live education and our first-of-its-kind
Foundations of Cardiometabolic Medicine Certificate Course.


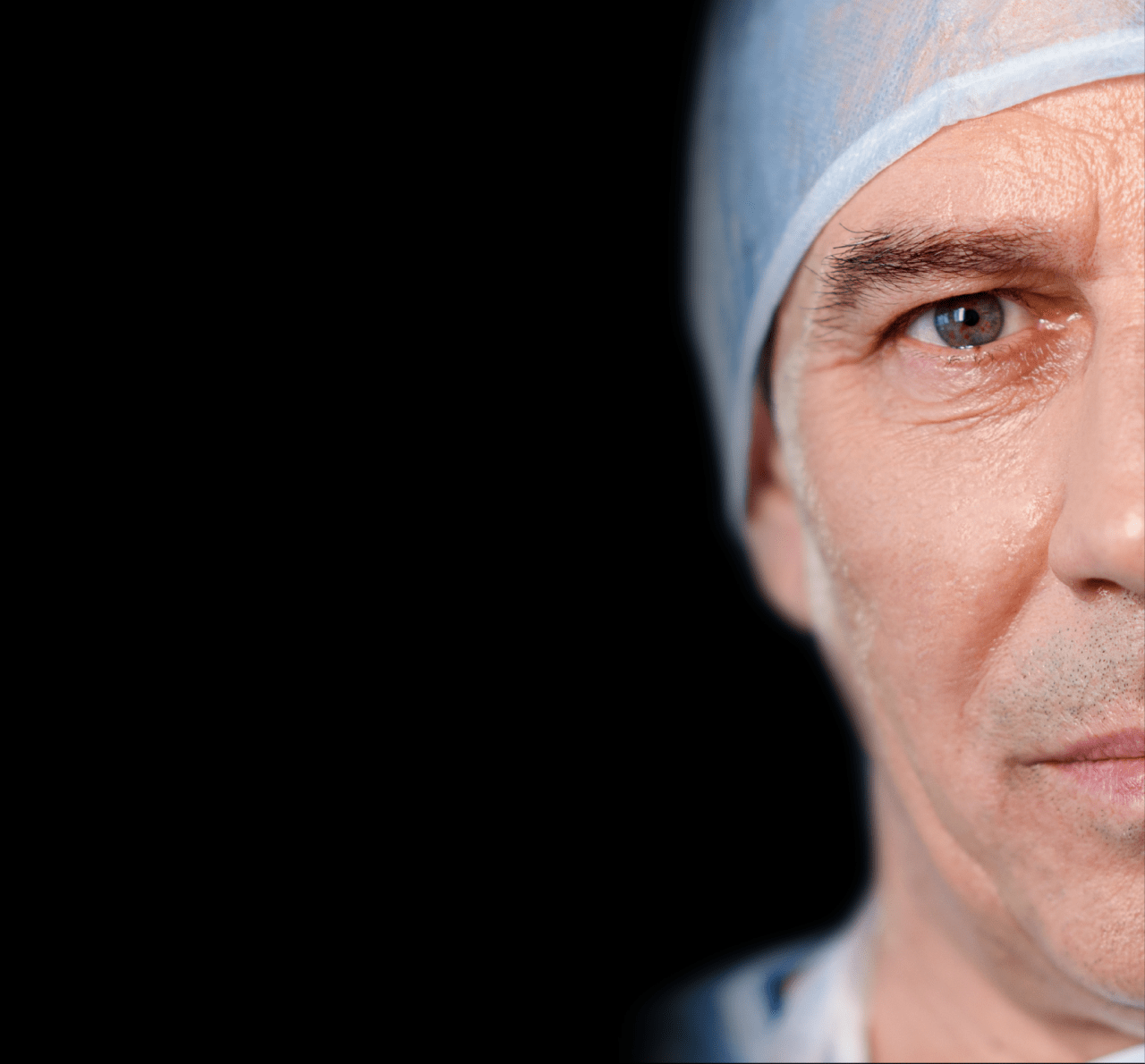
I knew I'd be seeing a mix of patients. Some patients would have serious and hard-to-treat endocrine disorders affecting their pituitary gland and growth hormones, resulting in developmental problems. I'd see women who were struggling with infertility, men with low testosterone, and patients of both genders with thyroid issues that lead to weight fluctuations and other health issues. Some adult patients who'd developed type 1 diabetes as children would be visiting me for ongoing management of a disease that, a hundred years ago, would have probably killed them in childhood. But today, if they can afford and access life-saving insulin, these patients can live long into adulthood. And, with new developments in continuous glucose monitoring devices and insulin pumps, their lifestyles don't differ that much from those of their nondiabetic peers.
All of these patients present unique clinical challenges; some diagnoses are textbook, but most of the time, I'm following a web of symptoms and patient-reported incidents that lead me to what feels like the satisfying end of a mystery novel. This is most true of my patients with the complicated comorbidities of overweight and obesity, prediabetes and insulin resistance, polycystic ovary syndrome (PCOS), and other metabolic impairments. For instance, a woman in her 20s presents with insulin resistance, PCOS, and a high body mass index (BMI). I must decipher whether her high BMI resulted in insulin resistance and years of glycemic instability resulted in her PCOS, or whether an underlying hormonal imbalance resulting in PCOS caused the weight gain, straining the endocrine system enough to affect insulin sensitivity. I will continue to solve these cases for my patients, but the global health crises of unaffordable insulin, inequities in access to health insurance, and racial disparities in access to any kind of care (but especially care from specialists like me) means that I'll never solve the whole problem. I enjoy my job, but I'm not equipped to resolve the mounting issues facing my patients, colleagues, and the public health community.
I am fighting an uphill battle that I can't win by myself. I am looking for a community of providers that can see the bigger picture and that will join forces to effect change, not just in daily practice but in health care policy.
